Anatomy
Calvin Coffrey
Ayhan Kuzu
More than a century ago
Surgery deep in the pelvis is difficult to perform due to limited working space which is mainly determined by the bony pelvis. At the level of pelvic inlet, midpelvis, and pelvic outlet, the diameter of the pelvis is more restricted in males than females. Gender therefore often plays a role in the difficulty level.
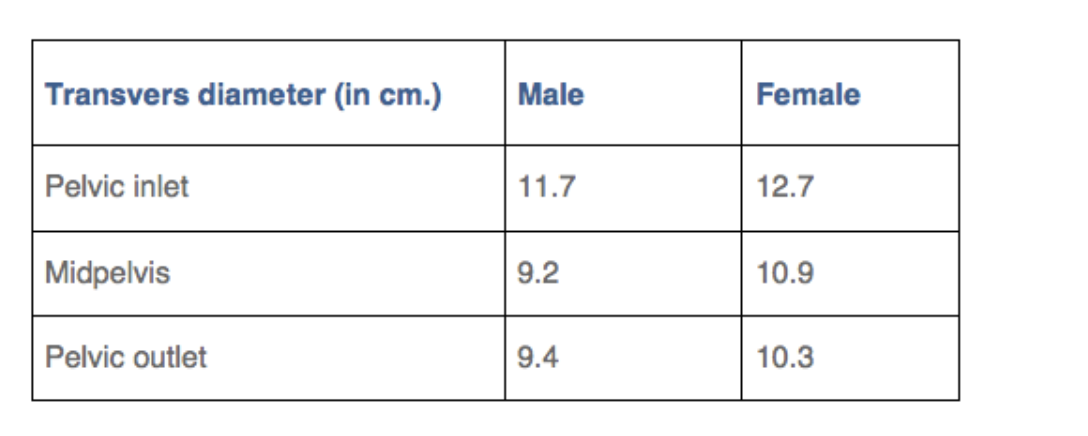
Factors affecting the difficulty of laparoscopic total mesorectal excision with double stapling technique anastomosis for low rectal cancer.
Akiyoshi T et al. Surgery 2009
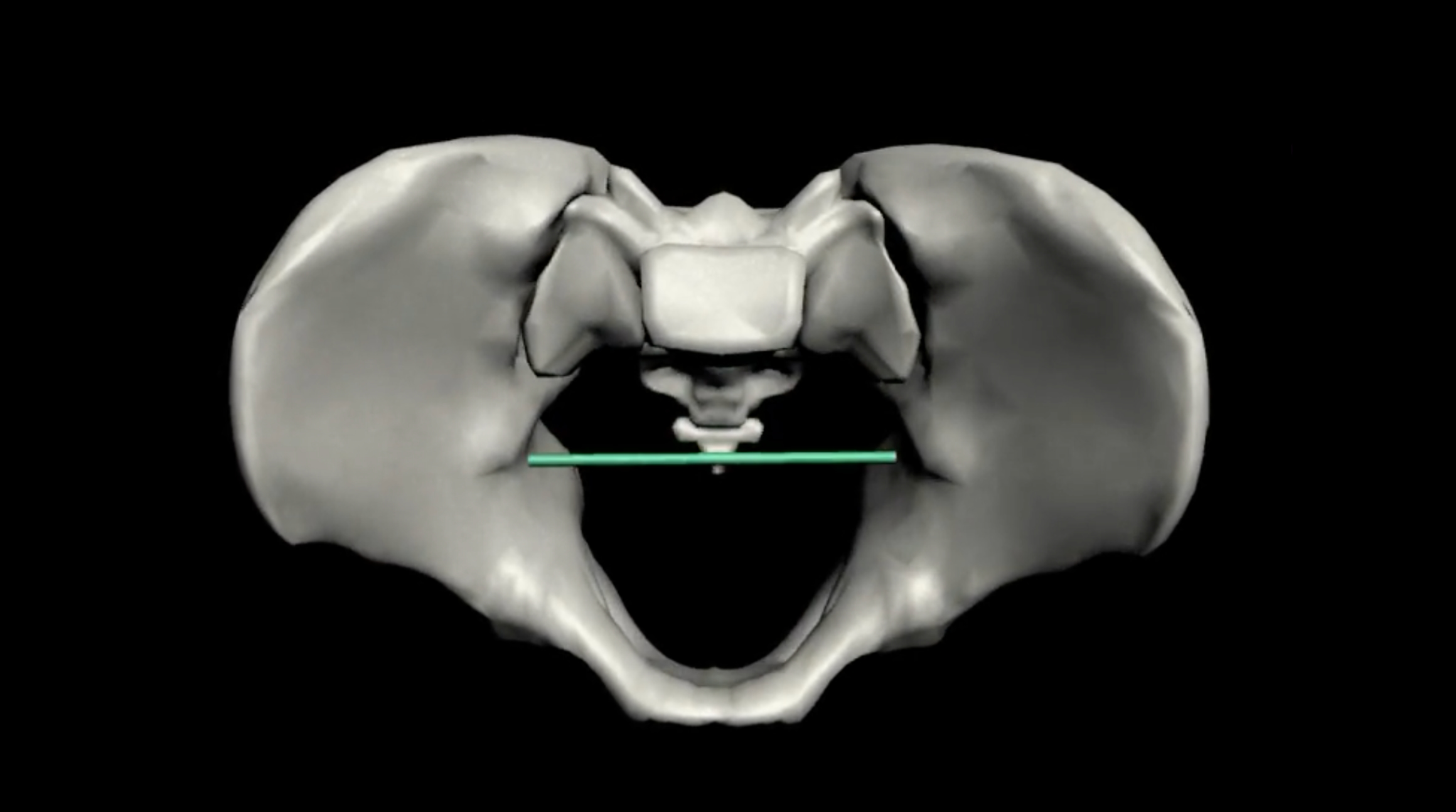
Animation showing the Pelvic outlet
Animation showing the Pelvic inlet
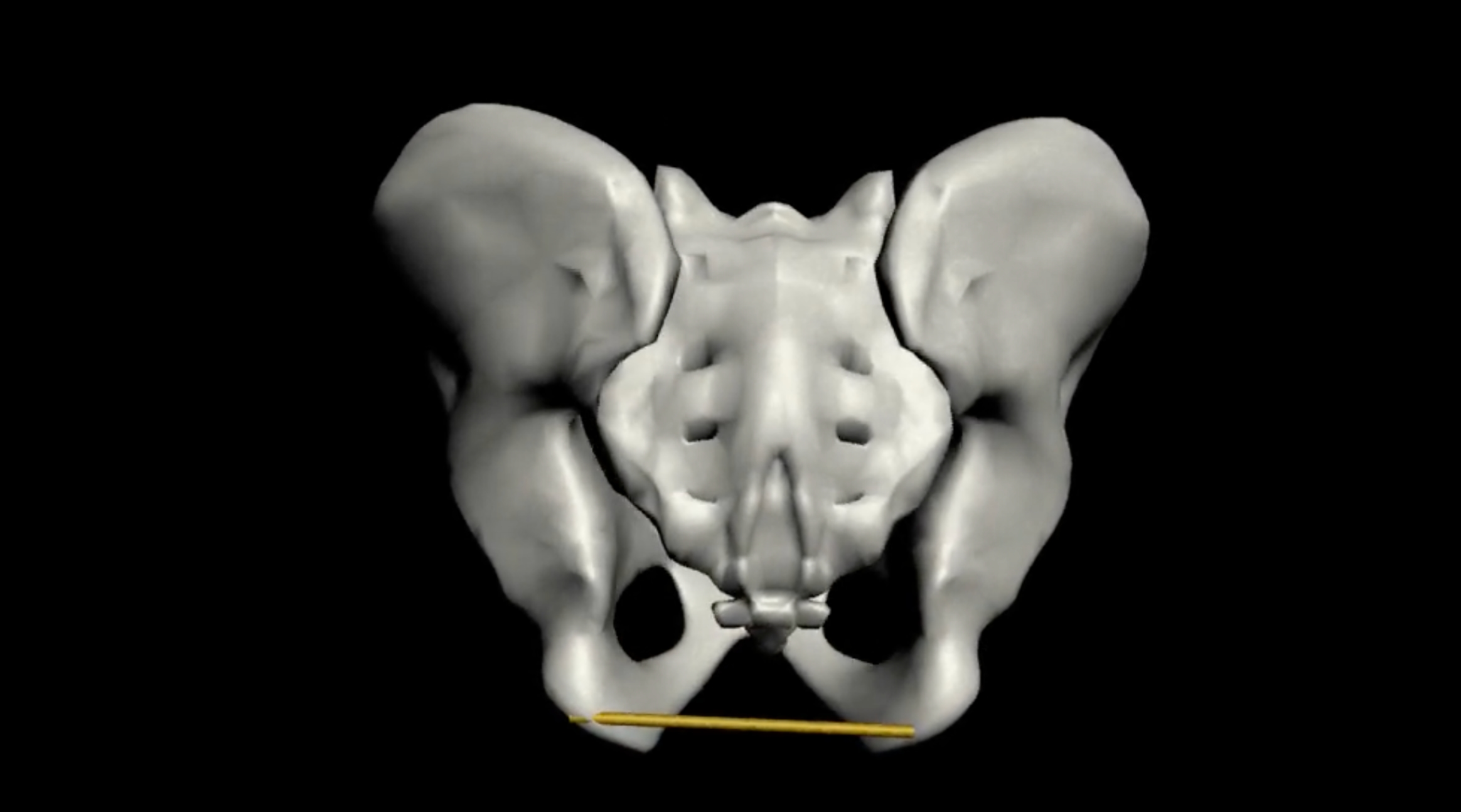
Furthermore, during the deepest part of the dissection, an enlarged prostate can further diminish the working space. This can lead to greater manipulation of the cancer specimen and a more difficult TME procedure in general
Schematic illustration of the pelvis with mesorectum (yellow) and prostate (green).
Dissection deep down in the pelvis becomes more difficult.
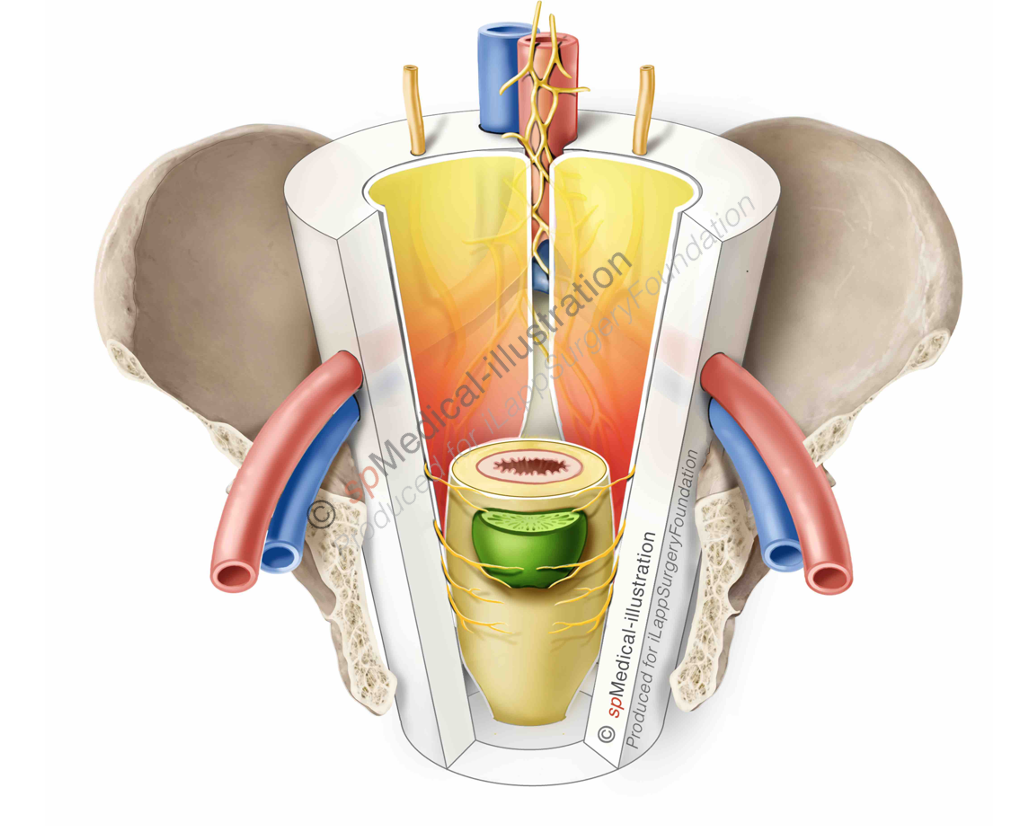
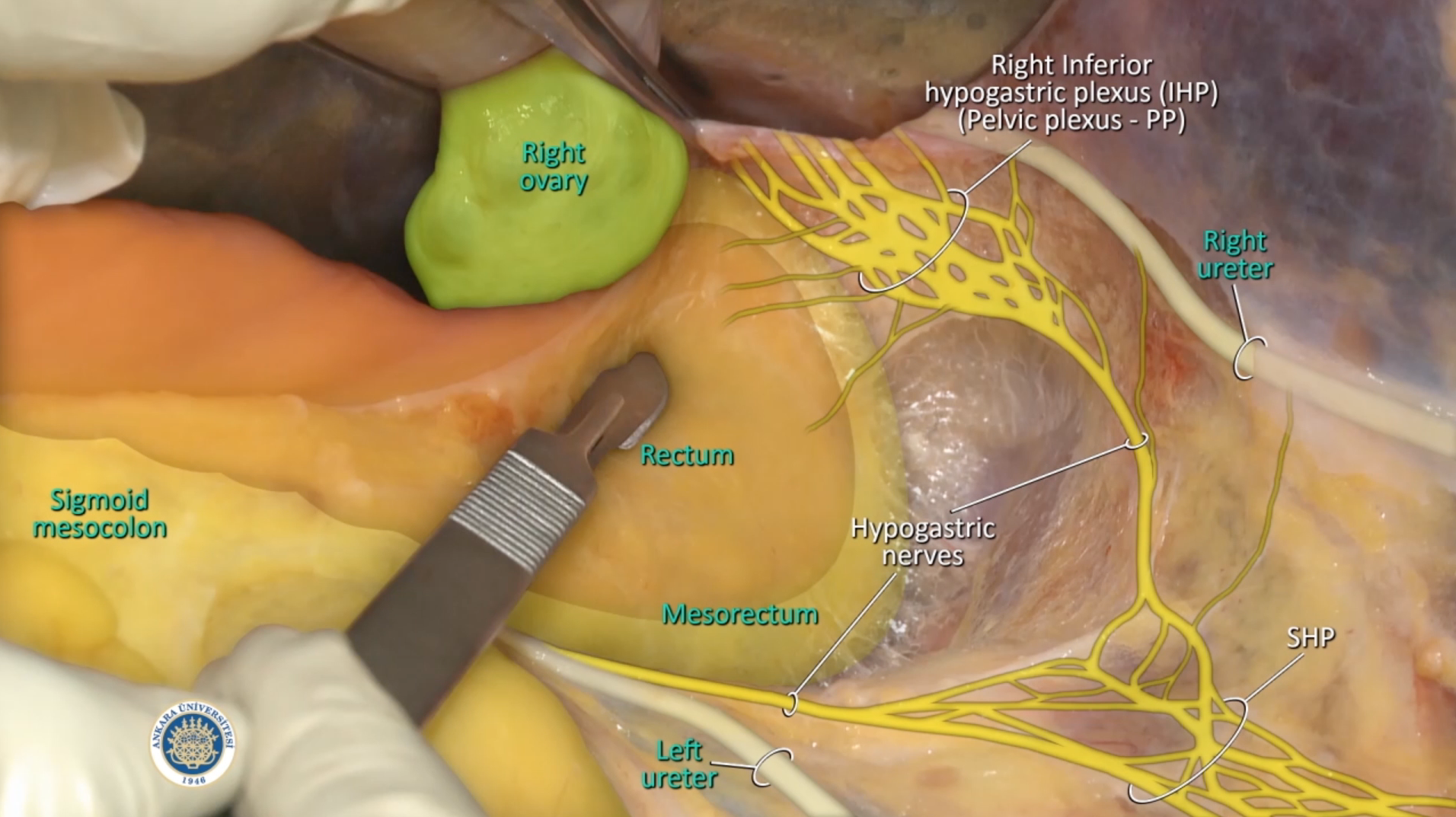
The shift from open rectal surgery to a laparoscopic or robotic approach had no impact on the view and orientation of the anatomy of the pelvis with all its delicate structures. The approach to the pelvic floor from above is well understood and the anatomic landmarks are well defined. Care must be taken to preserve important vessels and autonomic nerves.

The videos of Prof. Kuzu show the complexity of the anatomy of the pelvis. The rectum is shown as a midline evelope surrounded by paired structures, like nerves, vessels and ureters.
IMPORTANT: In the Anatomy chapter of the TaTME-procedure there is a lecture of Thilo Wedel included. Thilo discusses all aspects of the rectal anatomy, but with a focus on approaching the rectum from below.