Laparoscopic left hemihepatectomy
Ibrahim Dagher
P. Lainas
We hereby describe a standardized technique for laparoscopic left hepatectomy using identical steps as in open left hepatectomy:
- mobilization of the left liver
- dissection of the left hepatic vein
- dissection and prior control of the elements of the left hepatic pedicle
- parenchymal transection
- section of the left hepatic vein.
The dissection of the left hepatic vein is facilitated by image magnification provided by laparoscopy and by the Arantius approach previously described.1 In addition, laparoscopy considerably simplifies dissection and control of left portal elements.

Technique
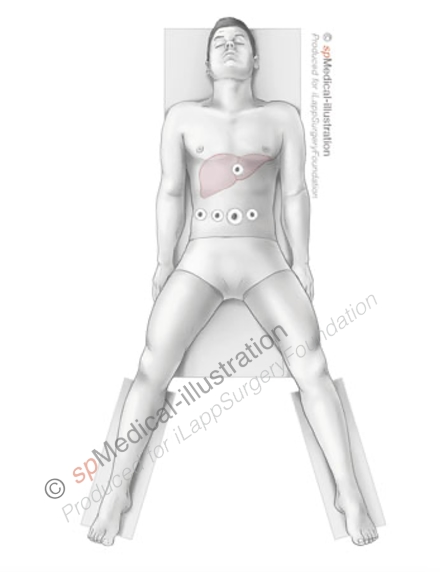
The patient is placed in a supine position, legs apart. The operating screen is placed at the head of the patient. The first surgeon takes position between the legs of the patient, with the second surgeon taking place on the right.
Five trocars are generally used (three 10mm placed centrally and two 5mm placed laterally), positioned in a semicircular line with the concavity facing the left hypochondrium. A 0° or a flexible tip laparoscope is generally used throughout the procedure.
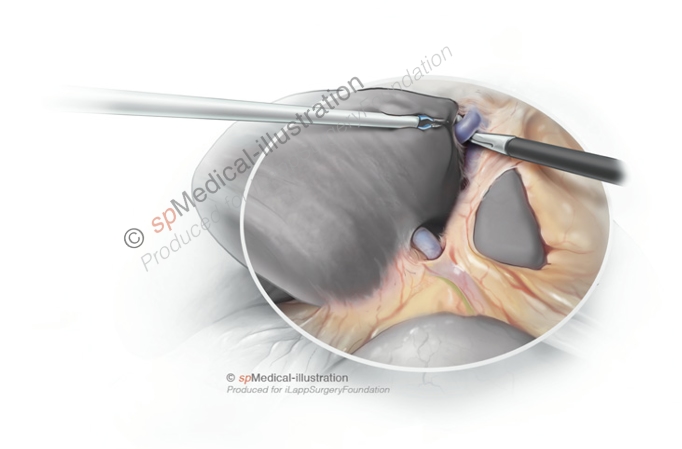
Left liver mobilization and control of the left hepatic vein
The left liver is pushed downwards after section of the round ligament and traction on it using a grasper. The first step of this approach is the section of the falciform ligament, the anterior leaf of the coronary ligament and the fatty tissue surrounding the anterior border of the hepatic veins. This dissection is performed handling the scissors in the right hand and bipolar coagulation in the left hand. The left triangular ligament is divided.
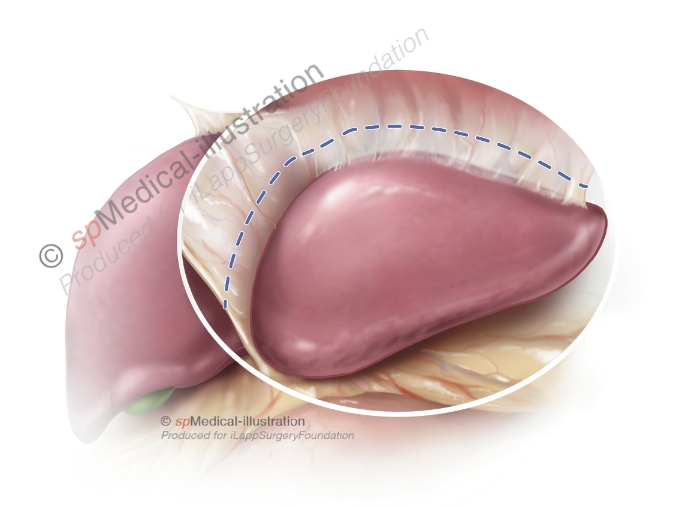
Then the left liver lobe is lifted to expose and identify the ligamentum venosum (Arantius’ ligament) separating the left liver lobe from segment I. The liver capsule is incised longitudinally anterior to the Arantius’ ligament which is gently pushed posteriorly.
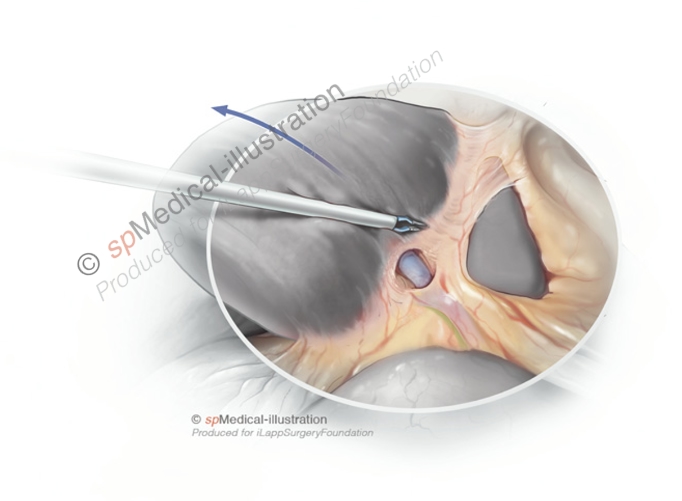
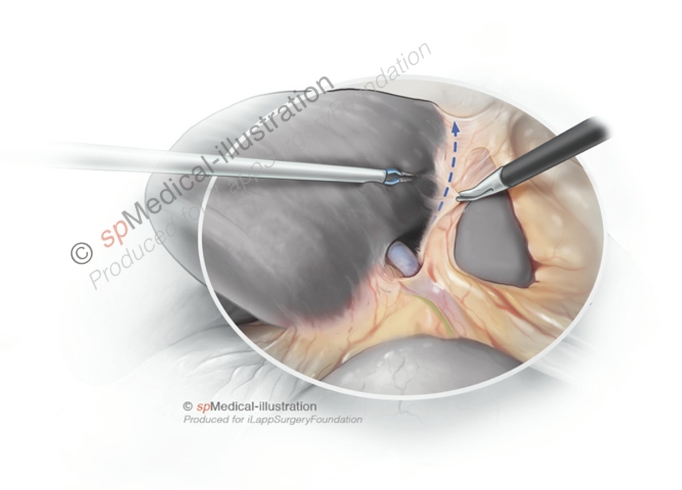
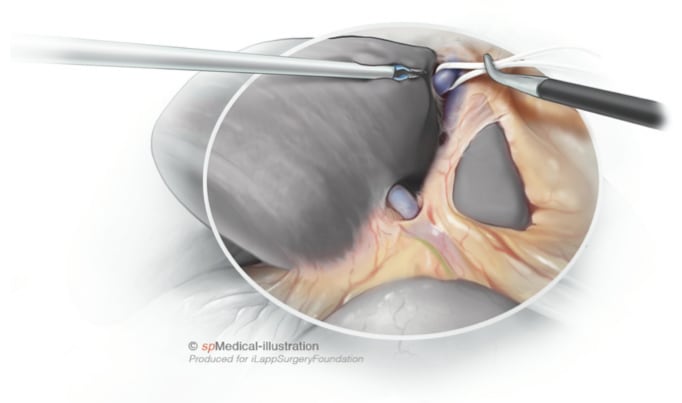
This dissection is conducted cranially in order to identify the inferior border of the left hepatic vein.
The space between the left and middle hepatic veins is dissected connecting with the superior part of the dissection, and a tape is placed around the left hepatic vein.
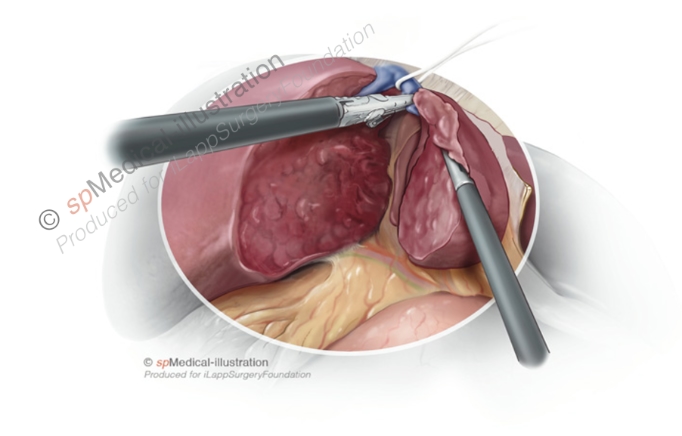
Extraparenchymal control of the left portal pedicle
The laparoscope is introduced in the middle trocar. Exposition of the hilar plate is achieved by traction applied on the round ligament and the gallbladder. The hilar plate is opened using scissors and bipolar coagulation is used cautiously for bleeding control during dissection. Dissection of the left hepatic artery and left portal vein is performed using scissors placed through a left hypochondrium trocar and bipolar coagulation through a right hypochondrium trocar. A small portal branch for segment IV close to the portal bifurcation is generally divided after bipolar coagulation. The left branch of the hepatic artery is sectioned after thermofusion or obstruction by clips.
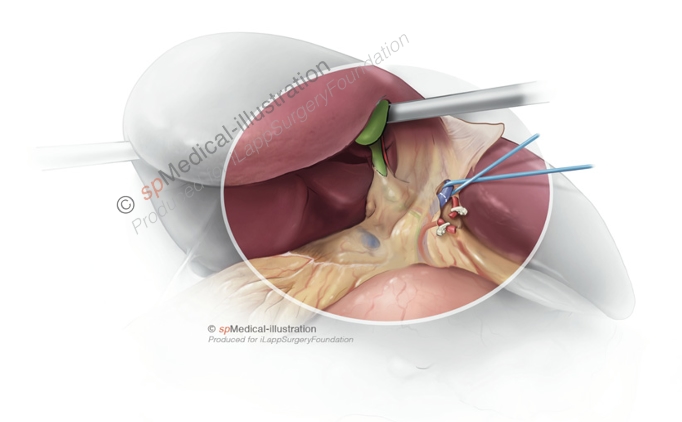
The left portal branch is dissected and sectioned using a vascular EndoGIA stapler. A small portal branch for segment I is generally identified and spared. The left hepatic duct is dissected and divided at the left extremity of the hilar plate, close to the round ligament, after obstruction by absorbable clips.
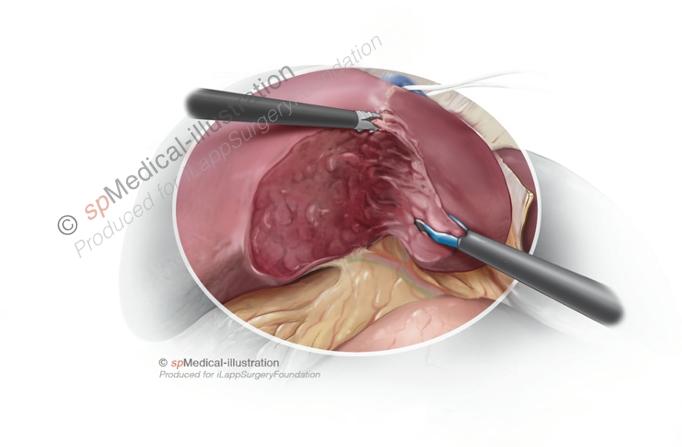
Parenchymal transection and left hepatic vein division
Parenchymal transection is performed using a thermofusion device. Absorbable clips are applied when necessary for hemostasis of large collaterals of the hepatic vein. At the end of the transection, the left hepatic vein is divided using a vascular linear stapler.
Extraction of the specimen
The resected liver is placed in an Endobag and extracted without fragmentation through a suprapubic incision or an existing abdominal scar.