Steps
Sami Chadi
Joep Knol
Although the transabdominal dissection can also be done open or robotically, we focus on the laparoscopic approach in this description. For the transanal part of the procedure, we limit this general description to the use of the flexible platform.

Transabdominal technique
The transabdominal portion is performed using a 4-port technique (5 or 10 mm port above the umbilicus, 5 mm ports in the left and right flank, and right iliac fossa). A 30° 10 or 5-mm camera is used for optimal visualisation. For splenic flexure mobilization, an additional 5 mm port may be placed at the right subcostal margin.
A low threshold should be used to perform splenic flexure mobilisation, and many surgeons will do this routinely. Because a reverse Trendelenburg position is preferred for this part of the procedure, it is usually performed as the initial step.
A standardised laparoscopic splenic flexure mobilization is described in:
Laparoscopic mobilization of the splenic flexure: the use of color-grading as a unique teaching tool. Knol J, Wexner S, Vangertruyden G (2015). Surg Endosc 2015; 29(3): 734-5
The patient is then placed in steep Trendelenburg and either sequential, or synchronized transabdominal and transanal procedures performed.
Especially in initial experience it is preferable to identify hypogastric nerves, iliac vessels, seminal vesicles or rectovaginal septum from the abdominal side, in order to standardise technique.
Transanal technique
A standard 30° laparoscopic camera and conventional laparoscopic instruments are used. Through the flexible platform, three trocars are introduced; one for introduction of the laparoscope and two additional working ports.
Information on use of rigid platforms will be added at a later stage.
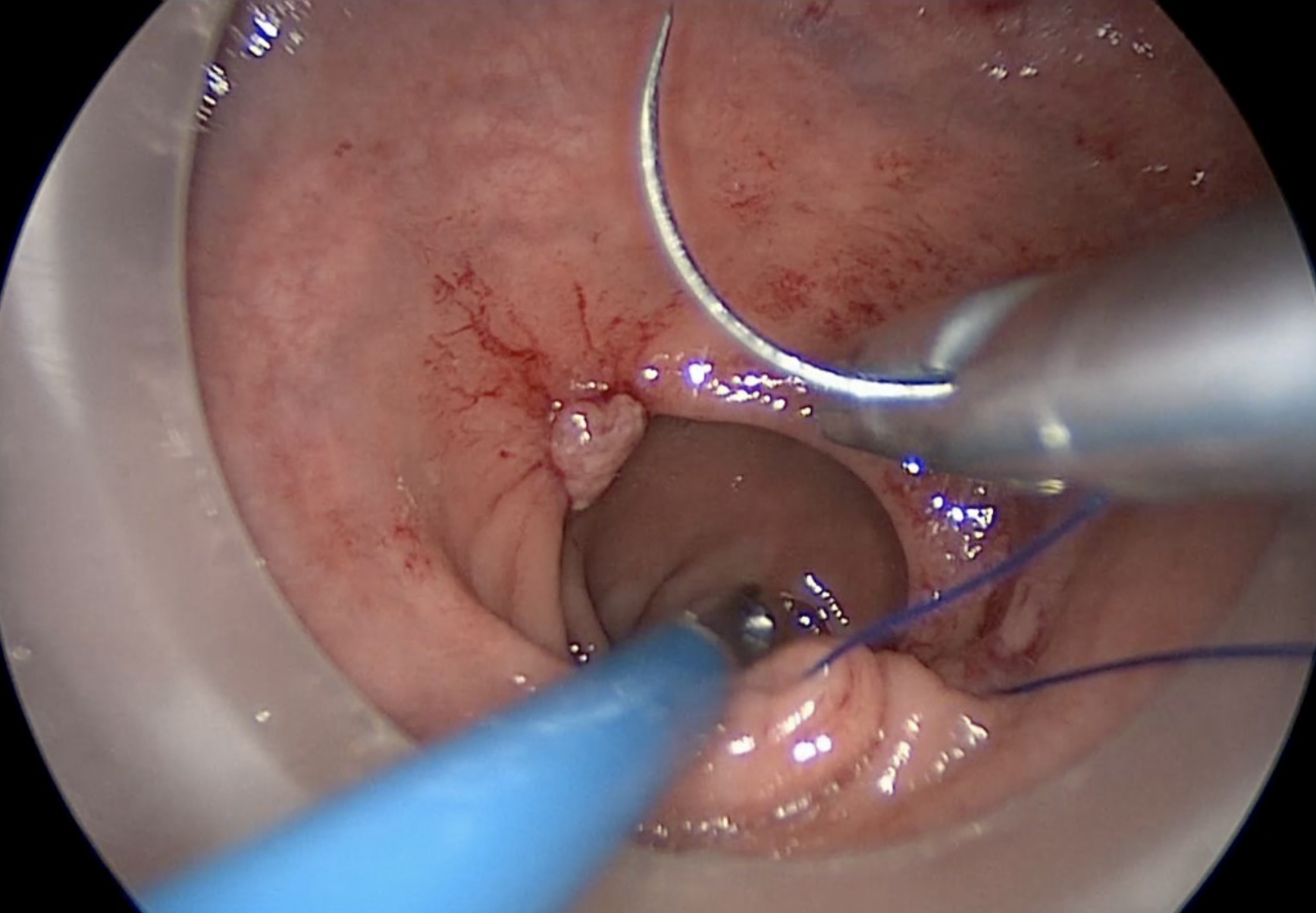
The placement of an 0 Prolene purse-string suture is the initial step of the transanal technique. It is placed from within the rectum to seal the lumen below the tumour, and to mark the distal resection margin.
Copyright Dr. Joep Knol
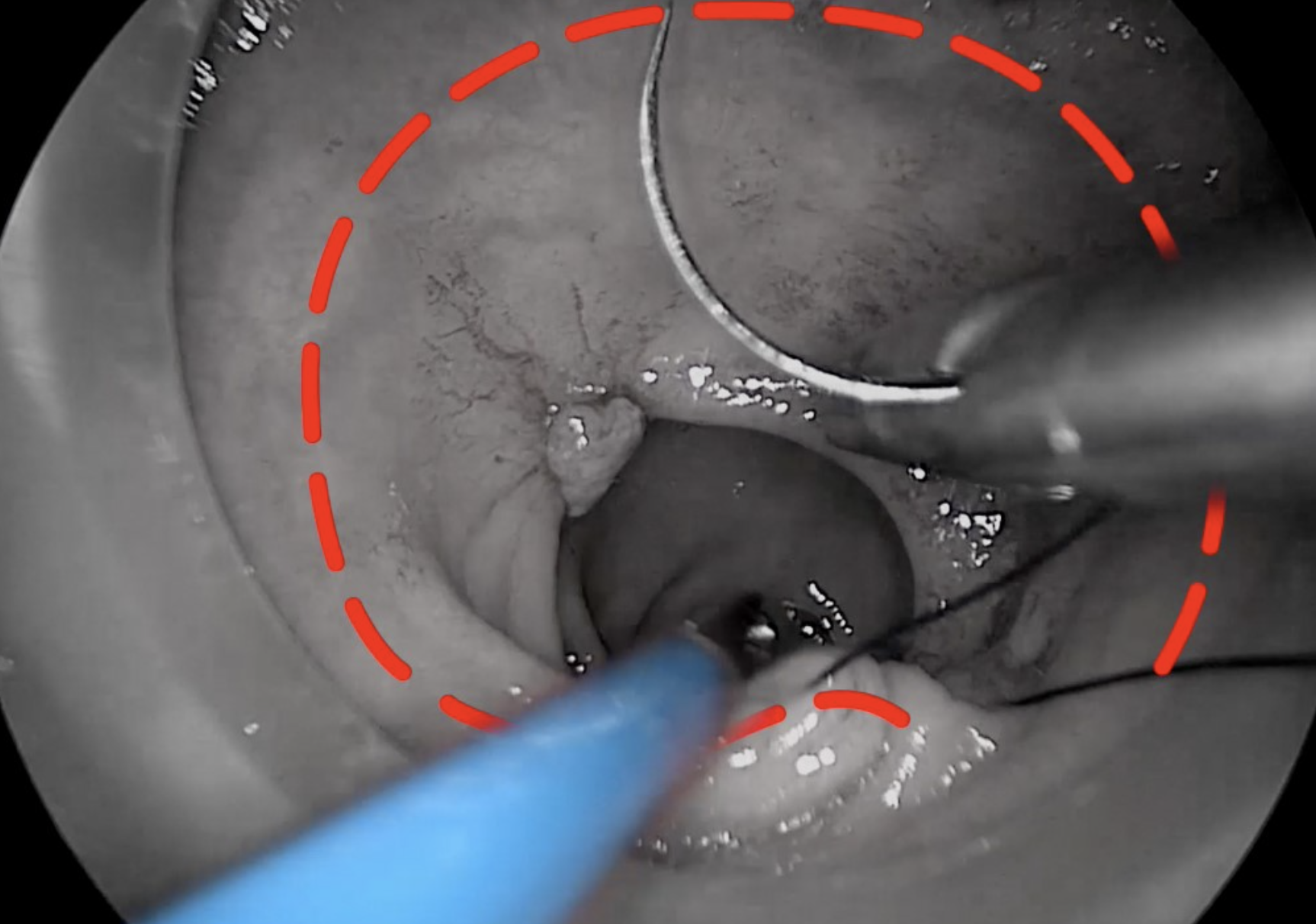
Placement of rectal pursestring. Note the dotted line indicating the accurate circumferential placement of the stitch below the lower edge of the tumour.
The pneumopelvis is then created using a standard laparoscopic insufflator or an Airseal-platform for a target pressure of 10-12 mmHg, with a 2-5 L/minute CO2-flow.
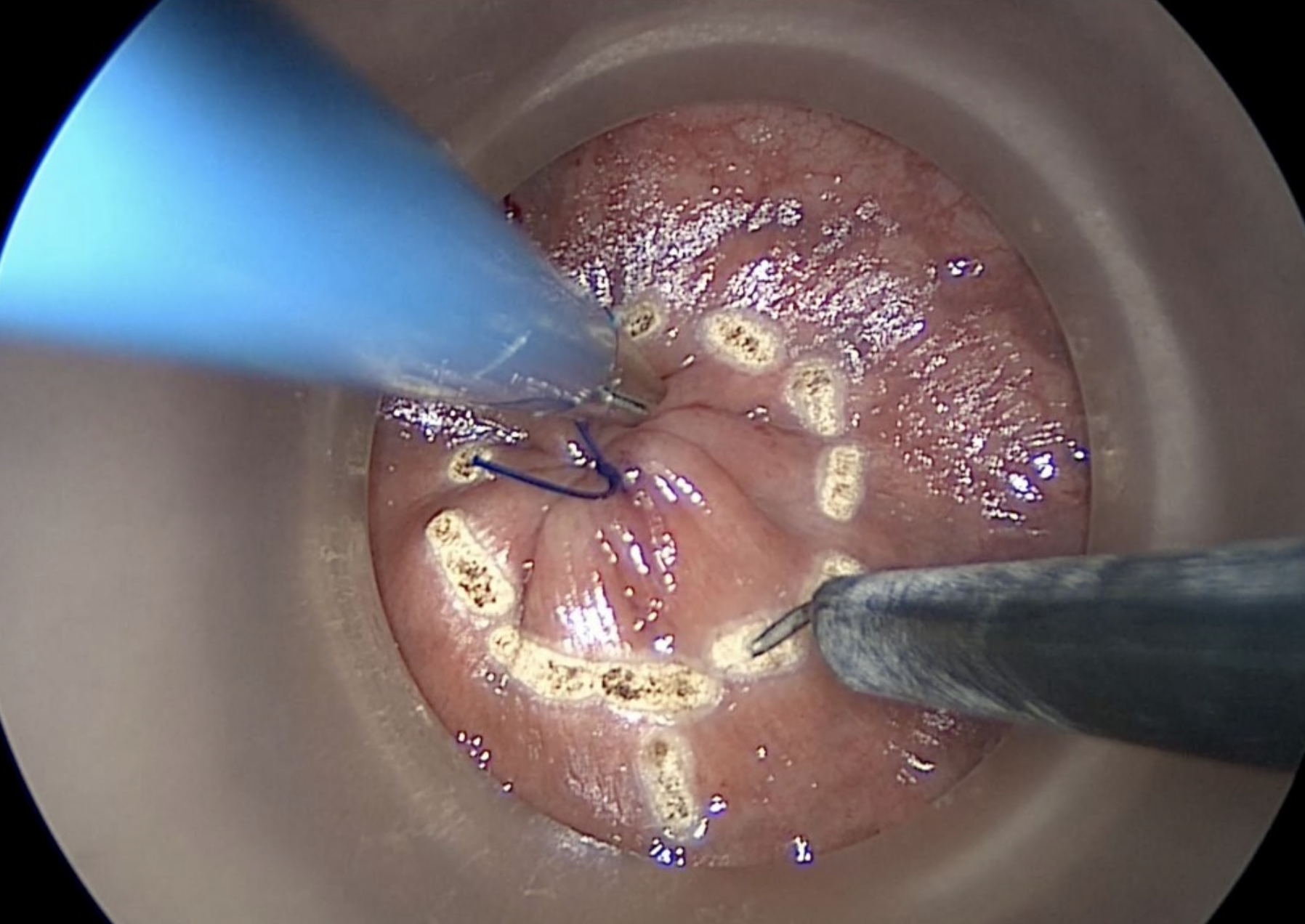
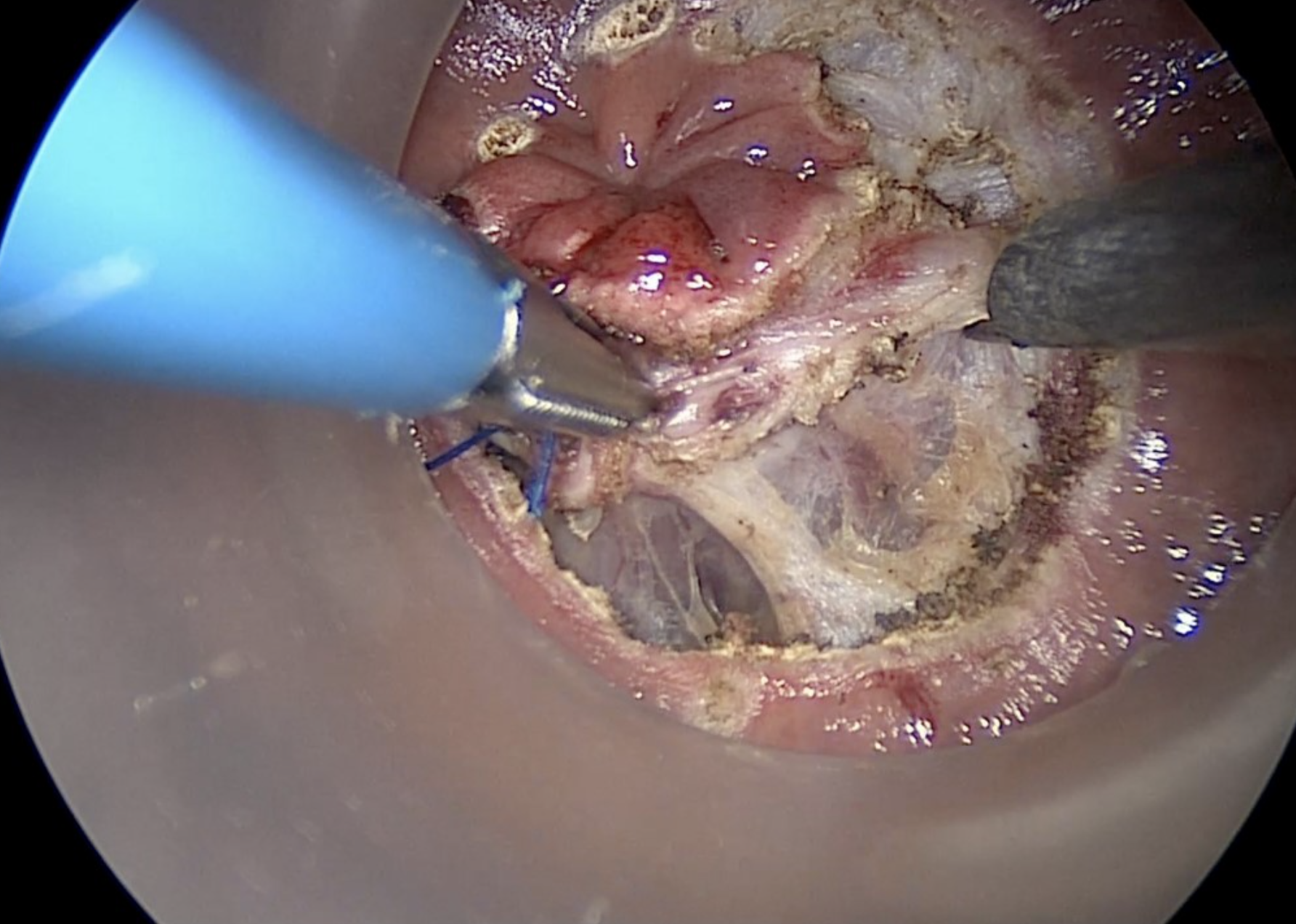
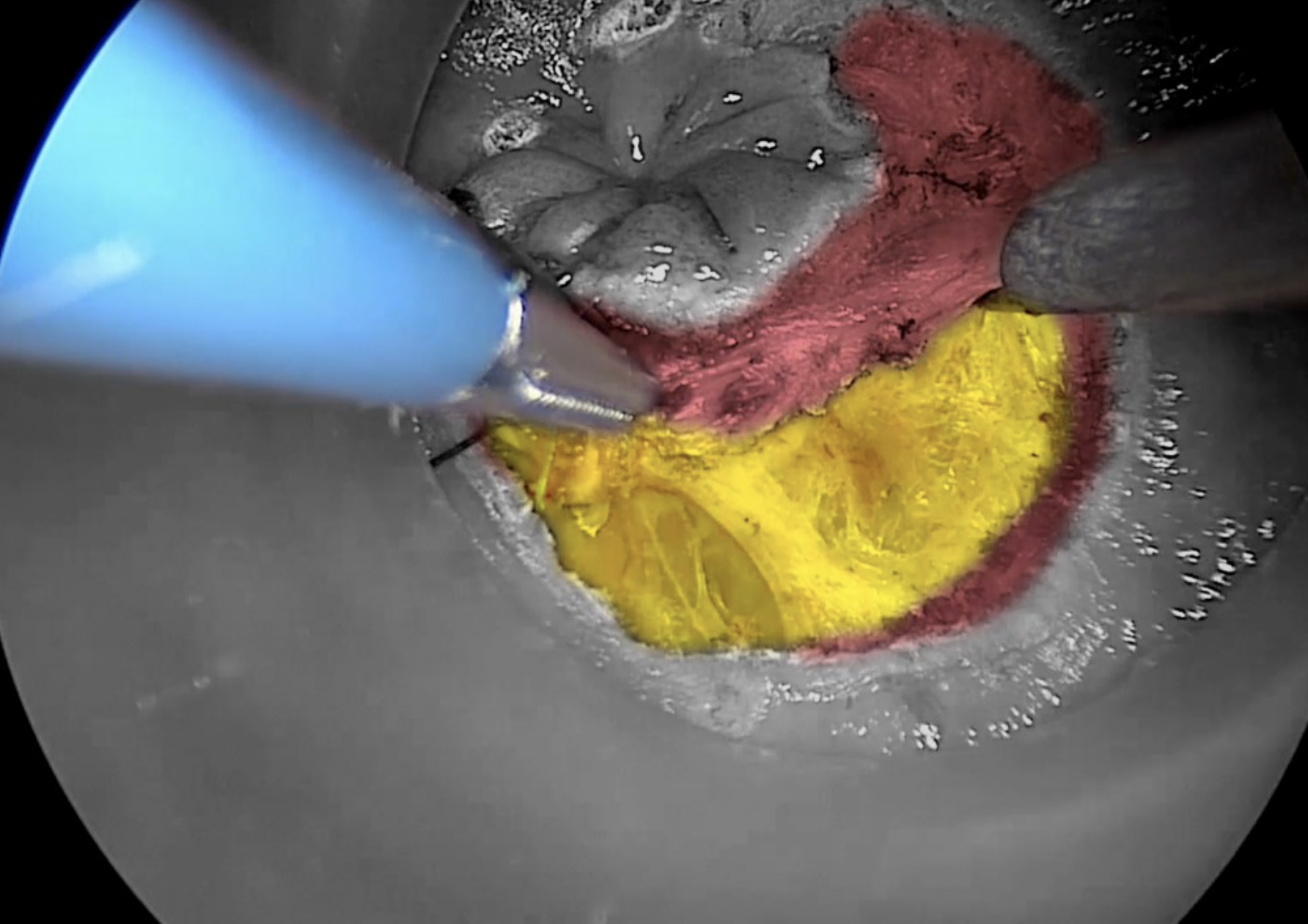
Before commencing dissection, it is our preference to mark the rectal mucosa circumferentially, using a conventional diathermy hook, just distal to the secured purse-string stitch. A full thickness incision of the rectal wall is started at the postero-lateral aspect, at either the 5 or 7 o’clock position.
Copyright Dr. Joep Knol
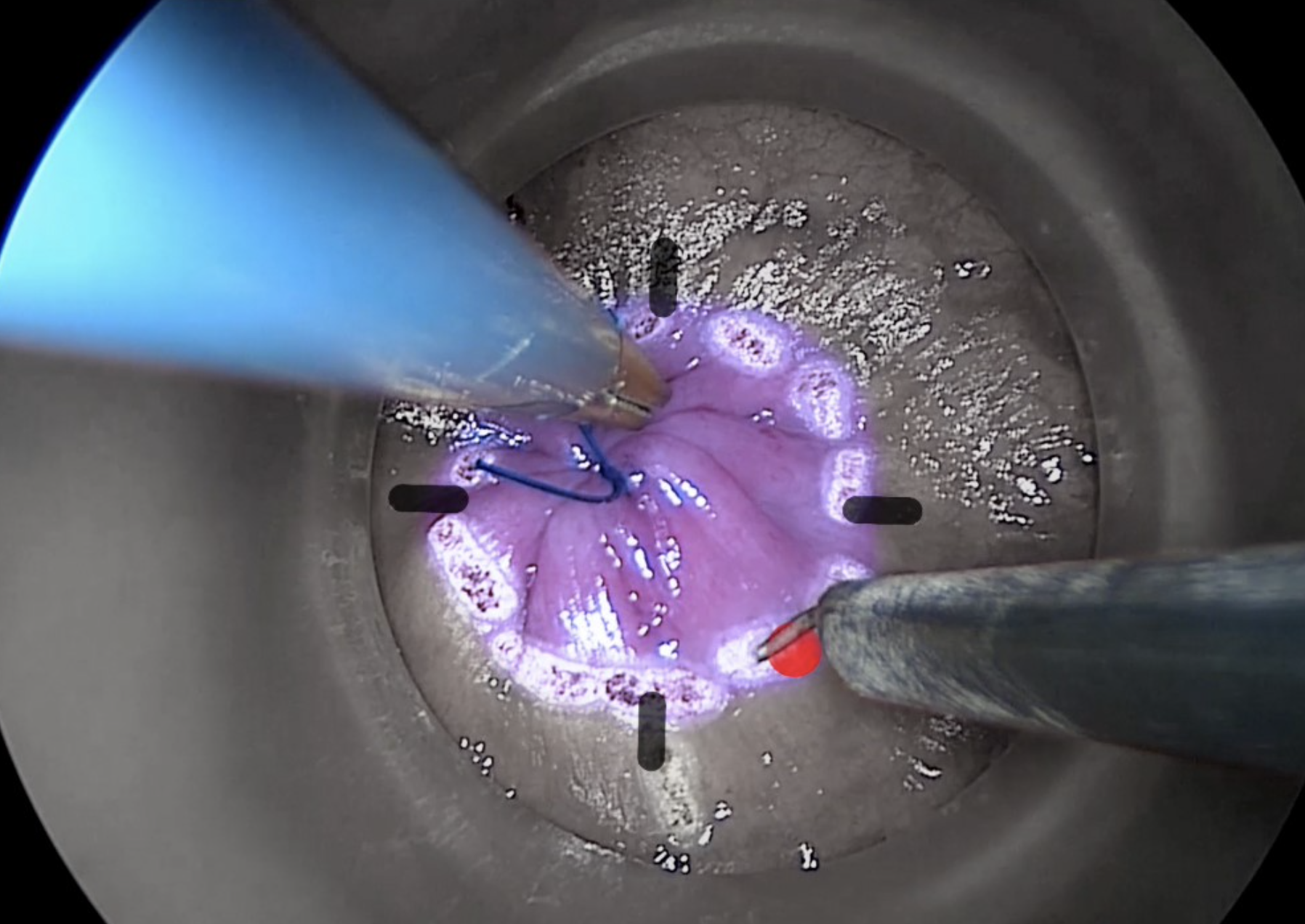
Diathermy marking of rectal mucosa to guide initial dissection. The contrast picture shows the distal rectal excision margin.
Using the hook diathermy, a full thickness incision of the entire rectal wall is completed.
Copyright Dr. Joep Knol
Diathermy hook dissection of the mesorectum, with yellow contrast showing entry into the correct mesorectal plane.
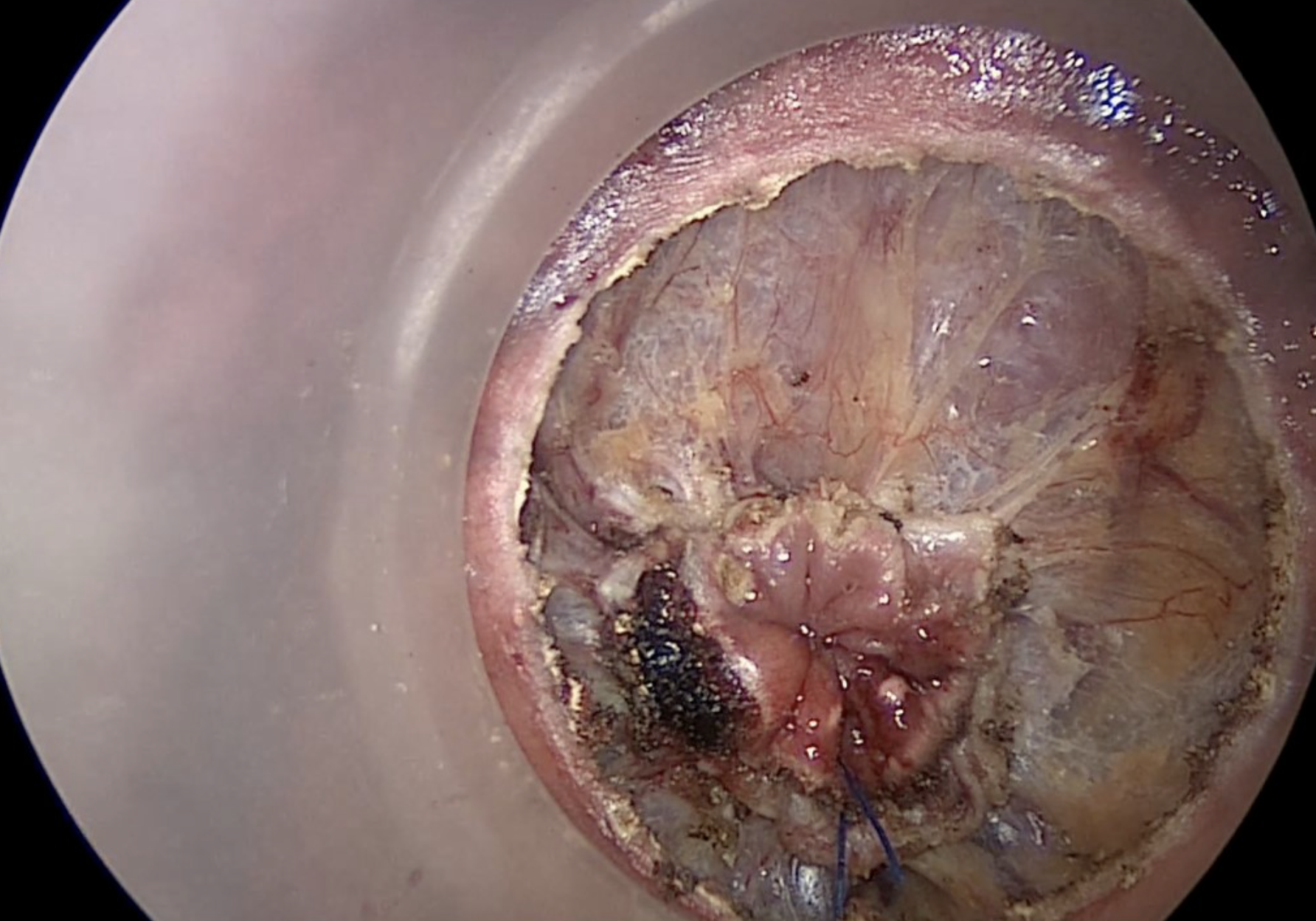
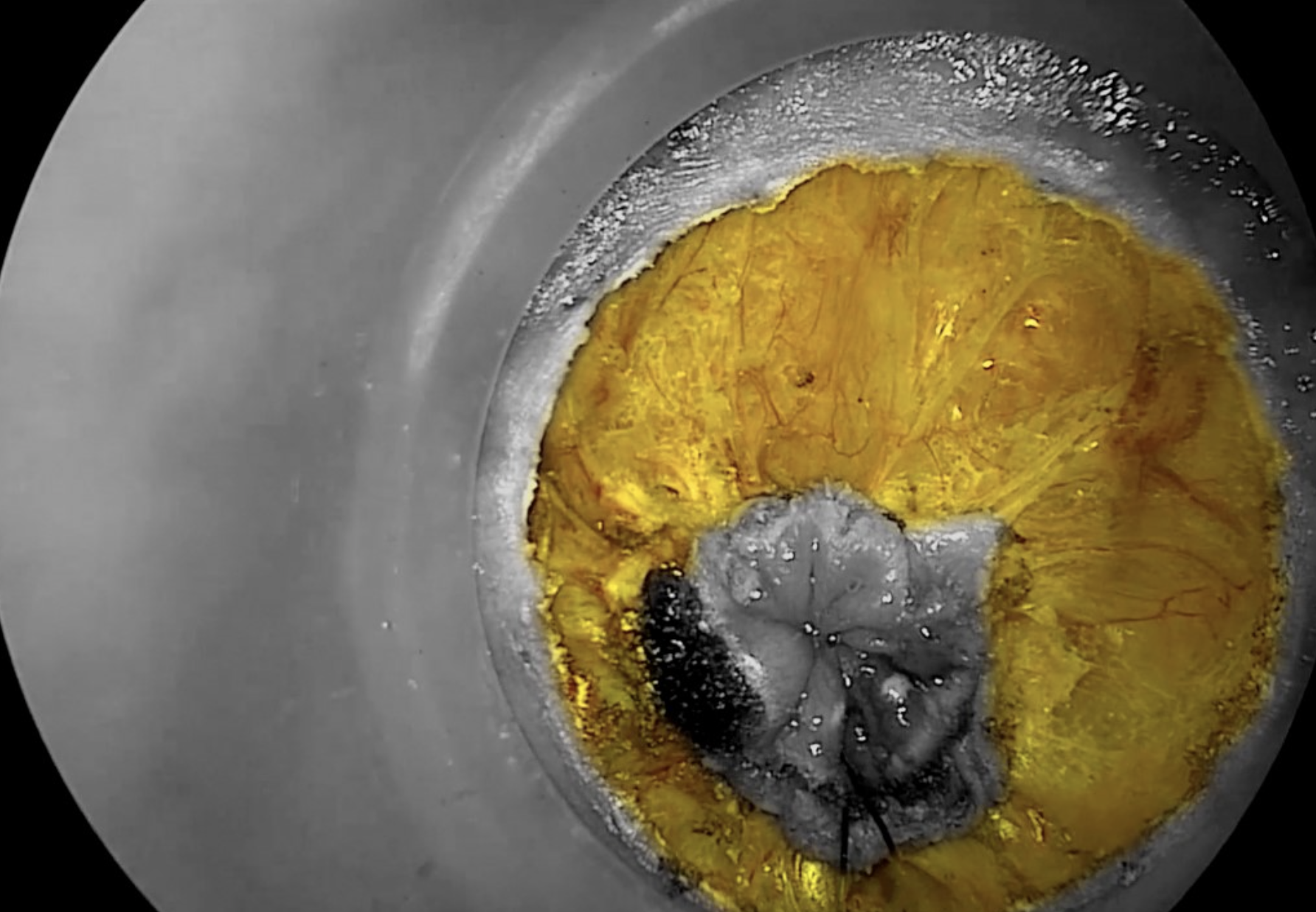
Circumferential entry into the correct mesorectal plane, highlighted in yellow.
The dissection proceeds in a standardized manner. Starting posteriorly, dissection is carried out perpendicularly through the rectal wall to the mesorectal fascia.
Dissection then continues up through the TME dissection plane both on the anterior and lateral side; in a synchronized dissection this can be done from both sides, and the last part of the lateral dissection can be facilitated by traction from both the abdominal and transanal surgeons.
The specimen is then extracted transanally or through the abdomen, depending on the surgeon’s choice.
Once the rectum is delivered, either abdominally or anally, then the proximal division can take place, often utilising a stapling device to seal the cut end of bowel.
Anastomosis
To reconstruct the bowel, a straight, end-to-side or J-pouch anastomosis is created, using either a hand-sewn technique or a stapled technique.