Difficult PS segments
Nonanatomical resections in the PS segments - Semiprone position
Mathieu D'Hondt
Laparoscopic liver resections (LLRs) for tumors in the posterosuperior segments are very challenging procedures. When the patient is placed in supine position, this area is located in the small subphrenic space (rib cage). LLs in this region requires manipulation and/or mobilization of the right hemiliver to obtain good vizualisation. Several techniques have been descriped to facilitate these complex LLRs:
- The hand-assisted approach
- The robotic approach with the use of articulating robotic instruments
- The use of intercostal ports
- Postural changes (left lateral position and semiprone position)

Intercostal port for anatomical segment 7 resection
In 2011, Ikeda and colleagues were the first group who published a paper on four right hemihepatectomies in semiprone position (1). In 2013, they published a larger case series of 30 laparoscopic resections in semiprone position including 11 major resections: 7 right hemihepatectomies and 4 posterior sectionectomies (2). In 2014 the same group published a paper in which they reviewed all patients who underwent a LLR from 2008 to 2013 at their centre .(3)
Since 2010 all patients with lesions in the anterosuperior segment (Segment 8), posterior segments (S6 and S7), and parts of the caudate lobe (caudate process and paracaval portion of S1) were placed in semiprone position. Before the introduction of the semiprone position 7 of 40 patients (17.5 %) with tumors in the anterosuperior and posterior segments underwent laparoscopic liver resection, and after introduction of the semiprone position, 69 of 120 patients (57.5 %) with tumors in the anterosuperior and posterior segments underwent laparoscopic liver resection (P<0.001). There were no conversions to open surgery, reoperations, or deaths. The semiprone group had a significantly higher proportion of patients who underwent partial resection or segmentectomy of S7 or S8, lower intraoperative blood loss, and shorter hospital stay than the supine group (all P\0.05). Postoperative complication rates were similar between groups. They concluded that LLRs in the semiprone position is safe and increases the number of patients who can be treated by laparoscopic surgery without increasing the frequency of major hepatectomy.
We recently published a comparative study comparing LLRs in the posterosuperior segments with identical open liver resections in the posterosuperior segments. (4) Laparoscopic cases were case-matched with those who had an identical open procedure during the same period based on tumor location (same segment) and the Brisbane classification of the resection.
Both groups were comparable for age, sex, ASA score, maximum tumor diameter, and number of patients with additional liver resections outside the posterior segments. Operative time was similar in both groups (median 140 min; p = 0.92). Blood loss was less in the LLR-group (median: 150 vs. 300 ml in OLR-group). Median hospital stay was 6 days in both groups. There was no significant difference in postoperative complications (OLR-group: 31.4% vs. LLR-group: 25.7%; p = 0.60). Patients undergoing LLR were treated with chemotherapy sooner compared to those undergoing open resection (41 vs. 56 days, p = 0.02). Our study suggests that laparoscopic parenchymal preserving liver resections in the PS segments can be performed with comparable short-term outcomes as similar open resections. The shorter interval to chemotherapy might provide long-term oncologic benefits in patients who underwent LLR.
In another paper we compared 25 LLRs in the posterosuperior segments in semiprone position with 20 laparoscopic left lateral sectionectomies. (5) Our results demonstrated that LLRs in semiprone for lesions in the difficult segments can be performed with similar
clinical outcomes as a minor laparoscopic liver resection except for longer operative time and larger intraoperative blood loss without the need for transfusion.
Semiprone position: step by step
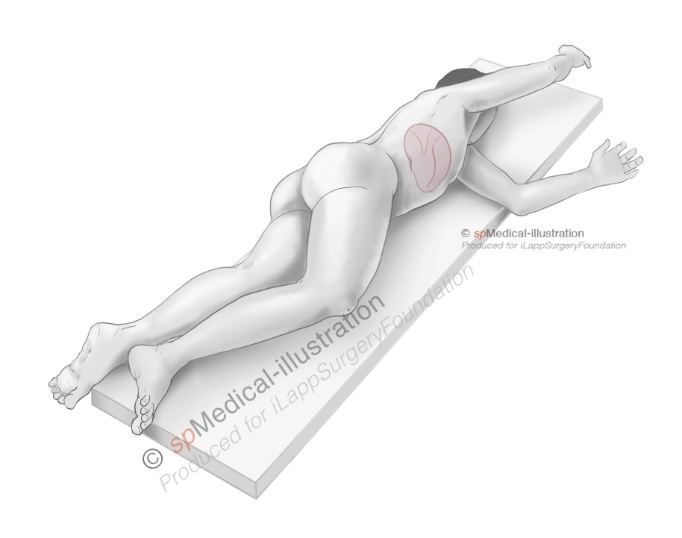
When positioning the patient in semiprone position, the patient is placed in a vacuum mattress in a left lateral position. The patient’s ventral surface should be on the edge of the table to allow the surgeon to move his laparoscopic instruments.
After being placed in the left lateral position, the table is “broken” to optimize the surgeon’s working space. Over-flexing the table should be avoided as this may limit the expansion of the abdominal wall and thereby limit the working space during the procedure.
Semiprone position
The patient is carefully anchored with tape or straps. All areas where tape or straps are applied should also be carefully padded. The patient should be anchored very securely, care should be taken not to anchor the patient tightly around the thorax as this can increase inspiratory pressures.
Once the patient is draped, the table is turned 30°–45° toward the semiprone position. The surgeon is positioned on the left side of the patient, but in some cases parts of the procedure are performed with the surgeon on the right side, for example a laparoscopic anatomical segment 7 resection.
Advantages of semiprone position
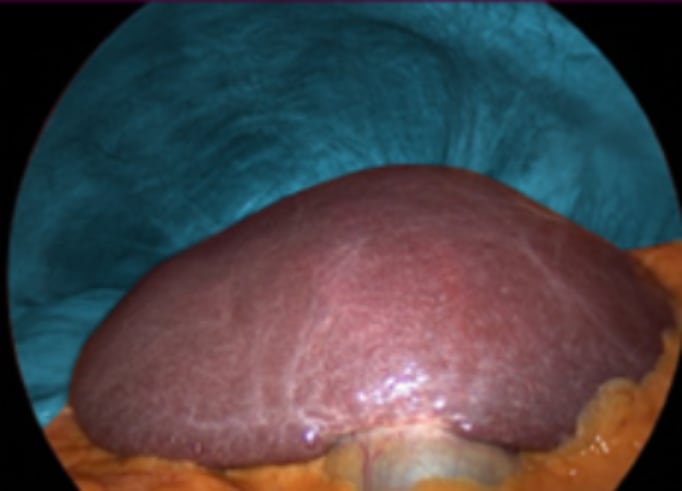
1. Other organs such as the transverse colon, stomach, and small intestine fall to the lower left while the liver stays in place (coronary /triangular ligaments). This is a big advantage for nonanatomical resections in segment 8 where mobilization of the liver is often unnecessary
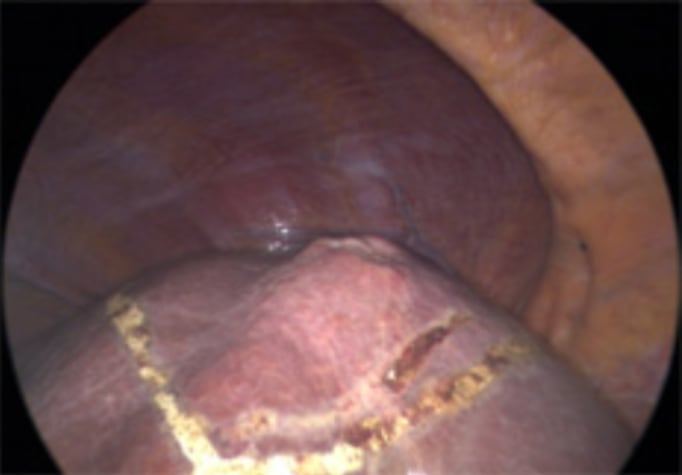
Nonanatomical resection for colorectal liver metastasis in segment 8. Without mobilizing the right hemiliver a good view is obtained.

Placement of stay suture
Nonanatomical resection using CUSA
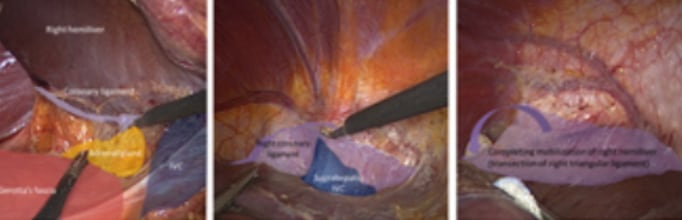
2. Semiprone offers a good view for right hemiliver mobilization
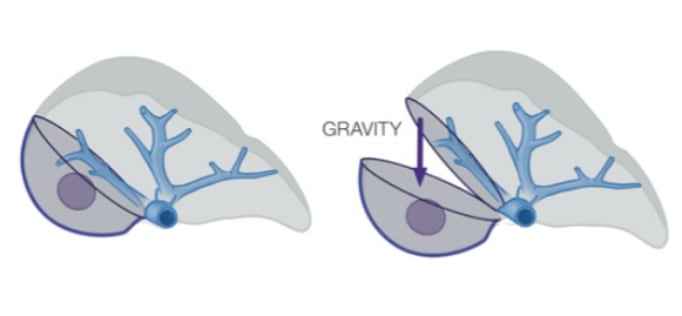
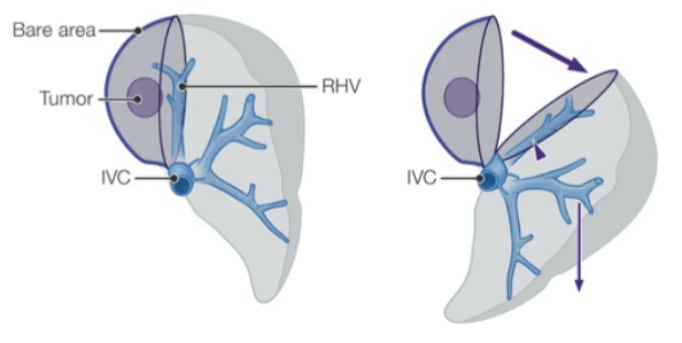
3. When the right hemiliver is mobilized, the right lobe slips to the left due to gravity and a large working space is created under the right side of the diaphragm. This large working space is in contrast to the small subphrenic space seen when a patient is positioned in supine position
4. In supine position the cutting plane between the anterior and posterior sectors of the liver is horizontal and gravity obstructs the exposure of the cutting plane in the small subphrenic space which causes difficulties in bleeding control. However, in semiprone position the cutting plane becomes more vertical
Supine
Semiprone
5. Blood flows to the lower left side of the abdominal cavity
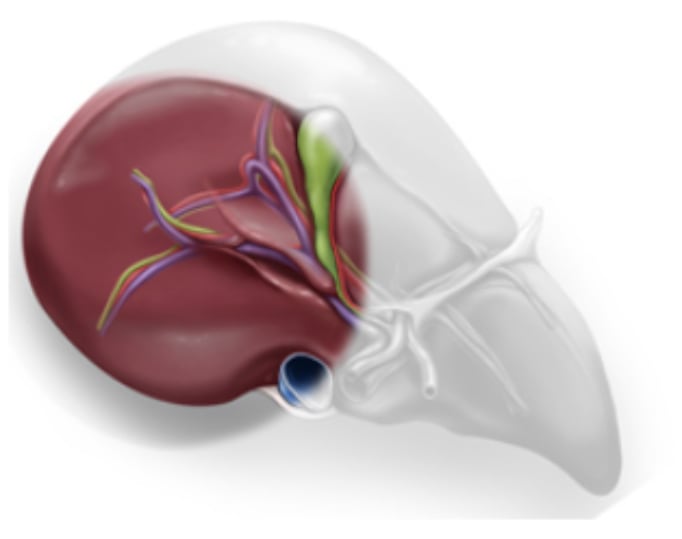
6. Semiposition offers better exposure of the right posterior segments and lifts the right hepatic vein higher than the vena cava to reduce hepatic venous bleeding (4)
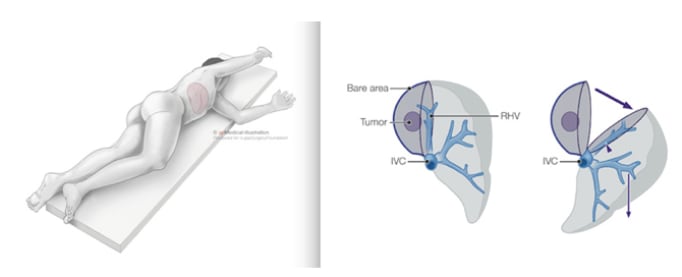
The right hepatic vein is higher than the vena cava: P (right hepatic vein) < P(vena cava)
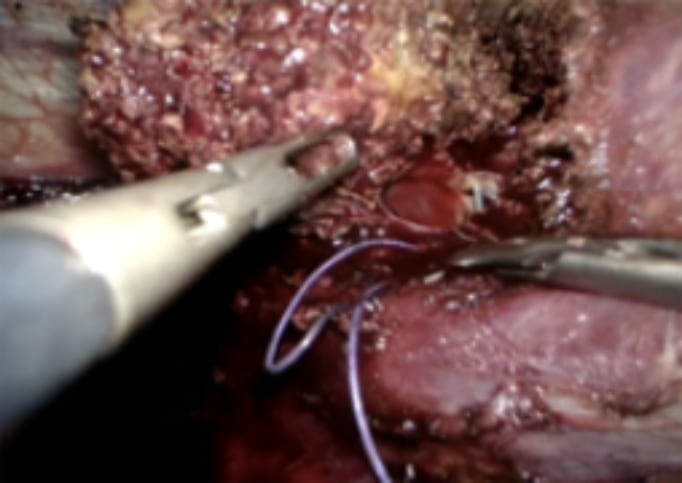
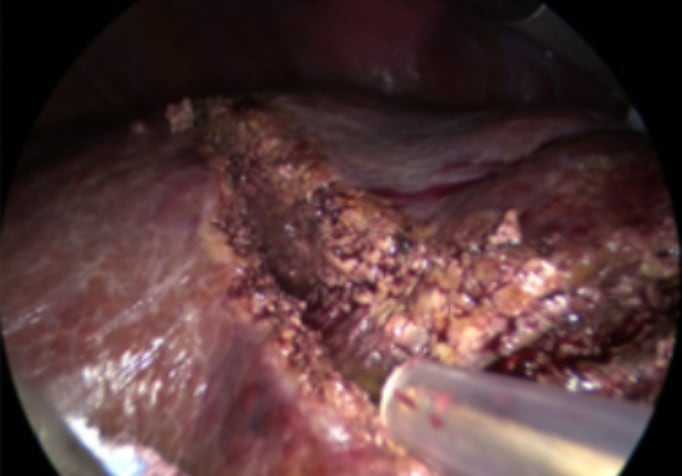
Picture showing large tear in right hepatic vein. The patient was positioned in semiprone. CVP during parenchymal transection was 8. Although CVP was relatively high, blood loss was minimal giving the surgeon time to suture the venous tear.
7. In semiprone position Rouviere’s sulcus is in the center of the operative field