Difficult PS segments : Laparoscopic posterior segmentectomy
Mathieu D'Hondt
As there are numerous reports about laparoscopic minor liver resections and left lateral sectionectomies, little is described about laparoscopic resections of the posterior segments.
Laparoscopic right posterior sectionectomy (LRPS) is a technically challenging procedure. The open approach remains the gold standard in many hepato-pancreato-biliary units.
In a recent worldwide analysis of more than 9,000 laparoscopic liver resections, only 1.2% cases were LRPSs (1). The Southampton guidelines for laparoscopic liver surgery define that there is a substantial role for laparoscopic surgery for resections in the difficult segments, as a laparoscopic approach is associated with less blood loss and a reduced hospital stay. Their consensus statement emphasizes the necessity of advanced expertise for surgeons undertaking resections in these difficult segments (2). Minimal working space, necessity for curvilineair parenchymal transection, difficulty in controlling bleeding from the tributaries of major hepatic veins and portal branches all contribute to the technical complexity of the operation. A posterior sectionectomy is the preferred choice for deep seated lesions in the posterior sector in proximity to or in contact with the posterior pedicle or lesions involving segment 6 and 7. Few studies studies have reported on the feasibility and safety of LRPS (3-5). In the recently paper from Siddiqi et al, the Southampton group described three different surgical techniques in their series of 29 LRPSs (5).
1. Ultrasound guided resection
The LRPS is performed without vascular control. The resection line is delineated 5–10 mm from the right hepatic vein while ensuring clear margin from the tumour. This was their preferred technique technique as it was performed in 69.0% (20/29) of the resections.
2. Rouviere’s sulcus exploration and inflow control
Rouviere’s sulcus is used to identify and control the inflow. The resection is guided by the ischemia line and IOUS. This technique represents 17.2% (5/29) of the resections.
3. Hilar dissection and inflow control
It consists of a hilar dissection and identification of the right posterior sectoral pedicle. The resection is guided by the ischemia line and intraoperative ultrasound (IOUS). This technique was performed in almost 14% of their cases (4/29)
Glissonean approach
The Glissionean approach was developed in an attempt to prevent extensive hilar dissection, reduce operative time and redice blood loss. (6-7) Launois and Jamieson standardized the technique and Machado described the technique for open and laparoscopic liver resections based on the studies of Galperin and Launois: the intrahepatic glissonian approach. (6-10) This technique precludes any dissections of the hilar plate. Small hepatotomies on the liver capsule over well-defined anatomical landmarks are performed to approach the pedicles, making dissection of the hilar plate unnecessary.
In laparoscopic liver surgery several reports have demonstrated the feasibility and safety of the Glissonean approach for left and right hemihepatectomy. (11-12) Considering the fact that a laparoscopic posterior sectionectomy presents special concerns about the extensive transection area which is often larger then in a case of a right hemihepatectomy, the Glissonean approach is often the preferred approach for these resections. The Glissonean approach allows safe and masse control of the portal structures of the posterior sector without prolonged dissection prior to parenchymal transection and resulting in less blood loss during transection. In an observational study, laparoscopic liver esection using the intrahepatic Glissonean approach was noted to have many advantages over standard laparoscopic liver resections including shorter operative time, lower transfusion rates, less margin positive resections, less morbidity and a shorter hospital stay. (13)
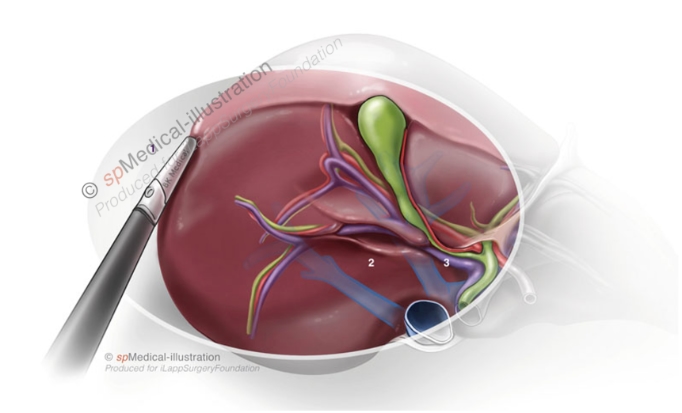
This approach is often possible since the the Glissonian sheath of the posterior sectoral pedicle is apparent inside Rouviere’s sulcus in 70% of cases. (14)
In a cadaver study, the frequency of the RS was 82% and in these the open RS was identified in 70% of the livers and the fused type was observed in 12% of the cases. In 18% of the livers no sulcus was found.

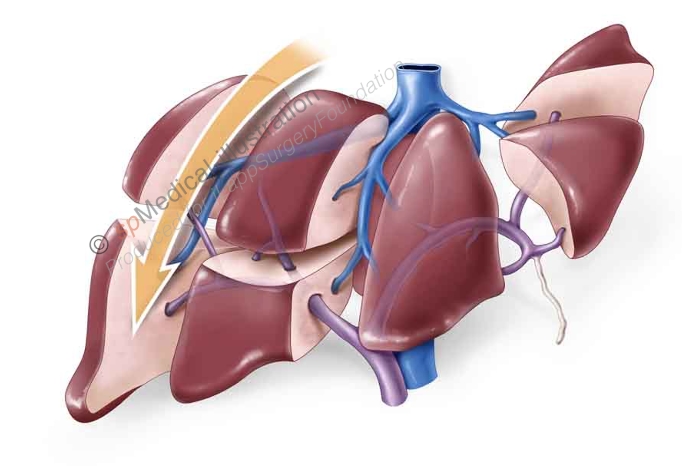
When performing a LRPS using the Glisonean approach two hepatotomies are made, one above and one beneath Rouviere’s sulcus.
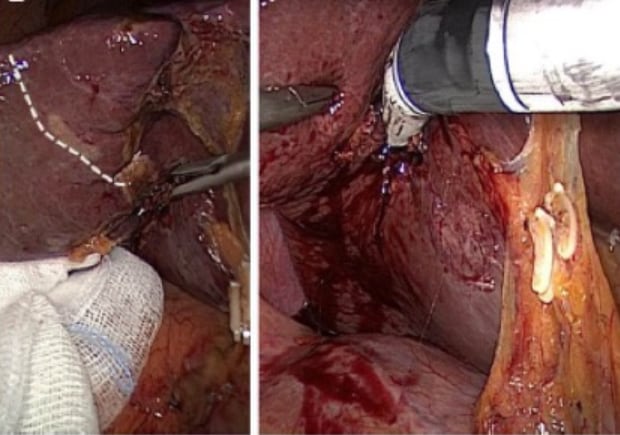
After test-clamping demarcation of the posterior sector is observed. The posterior Glisson’s pedicle is then divided en masse using a linear vascular stapler. The superficial hepatic parenchyma is transected using an ultrasonic scalpel or bipolar sealing device and the deeper portion of the parenchyma is transected with a laparoscopic Cavitron ultrasonic surgical aspirator. The small branches of the hepatic veins are controlled with endoclips or vessel-sealing instruments. The large branches of the right hepatic vein are clipped. The the origin of the right hepatic vein is transected with a vascular stapler when resection of the vein is necessary (depending on proximity of the tumor).