Introduction to difficult posterosuperior segments
Mathieu Vandeputte
Mathieu D'Hondt
Since the first international consensus conference (ICC) of Louisville in 2008, laparoscopic liver resection (LLR) has been spreading globally. Six years later the second ICC in Morioka in 2014 determines that minor LLR is confirmed to be a standard practice, since it has shown comparable short- and long-term outcomes with those of minor open liver resection (OLR). However, major LLR is still considered as an innovative procedure. (1)
Accumulated evidence indicates that LLR provides similar or better perioperative outcomes than OLR in terms of operative time, estimated blood loss, complication rate, and hospital stay. (2) Regarding survival outcomes, the literature indicates that LLR has overall survival and recurrence-free survival equivalent to those of open procedures. (2,3)
In the uprising era of laparoscopic liver surgery, a focus of attention is increasingly drawn to the resection of the posterosuperior segments, i.e. Couinaud segments 4a, 7 and 8.
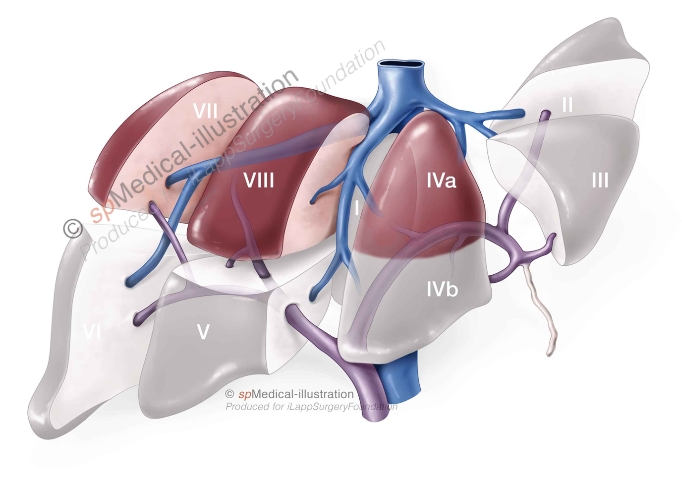
The posterosuperior segments
Until 10 years ago, the posterosuperior segments were traditionally not accessible for laparoscopic resection, due to technical difficulties. The principal issues include limited access and exposure, bleeding control and determination of a safe resection margin.(4,5) Additionally limited access of the portal triad and difficult pedicle control can occur.(4) Therefore lesions in the posterosuperior segments were poor indications for laparoscopic resection.
Only a few expert centers around the world with advanced experience in HPB surgery started with LLR of these segments. Technical evolutions, i.e. advances is laparoscopic devices, improved surgical skills to overcome the technical difficulties and growing experience of major LLR made it feasible to perform LLR in the posterosuperior segments.(5) Today, an increasing number of experienced HBP surgeons is performing LLR in these segments.
Laparoscopic resection of the posterosuperior segments is conventionally defined as a minor LLR according to the Morioka statement.(1) This, however, does not take into account the technical complexity of resections within the posterosuperior segments (4a, 7 and 8), and hence it was proposed that these resections be classified as technically major resections to differentiate them from minor resections and acknowledge their difficulty.(6,7)
Exposure of segments 7 and 8 to maximize the operative field can be enhanced in different manners. A recent systematic review distributes the different approaches in 3 categories: the lateral, the thoracoscopic and the transabdominal approach.(8)
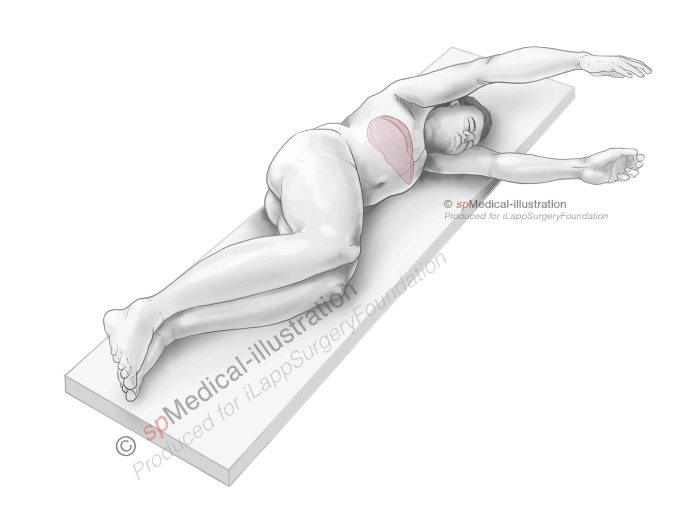
Lateral approach
Thoracoscopic approach
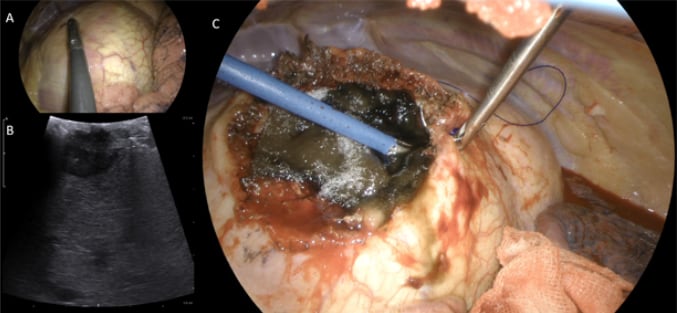
Patient underwent second repeat liver resection for colorectal liver metastasis in segment 8. Previous two parenchymal sparing liver resections were performed open. A and B: Detection of CRLM through the diaphragm. C: Closure of diaphragm after resection.
The lateral approach is most frequently chosen, according to this systematic review, and includes the transdiaphragmatic, transthoracic and intercostal approaches. The common advantage is that segments 7 and 8 are being approached from the cranial side. Careful consideration is required for possible pulmonary complications due to the risk of penetration of the diaphragm and thoracic cavity.(8)
The transabdominal approach requires full mobilization of the right liver lobe to reach the posterosuperior segments. Compared to thoracoscopic techniques, transabdominal approaches have the advantage of the pneumoperitoneum to reduce bleeding.(8)
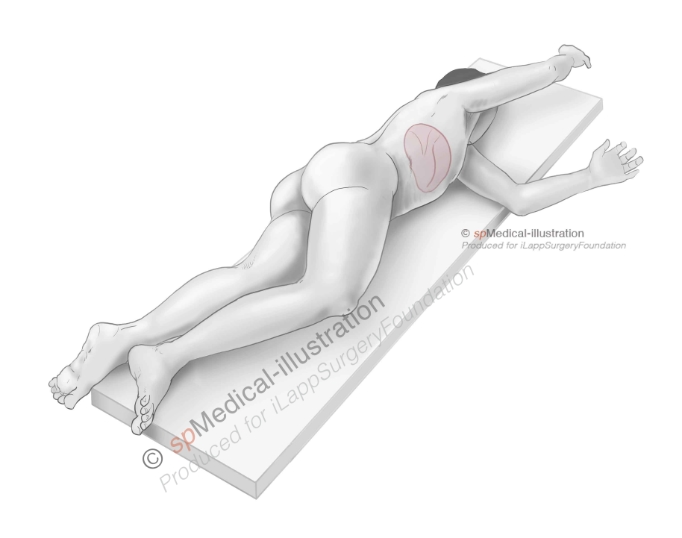
Semi-prone position is an interesting type of transabdominal approach, which uses the weight of the right lobe of the liver to expand the field of view, facilitating the mobilization of the liver. Semi-prone position offers better exposure of the posterosuperior segments and lifts the right hepatic vein higher than the vena cava to reduce hepatic venous bleeding (5,9,10) . Another advantage of semi-prone position besides the enhanced visualization, is the improved surgeon’s ergonomics.(10)